If my memory serves me correctly, I have been to an emergency care facility twice in my life. Unlike my brother, who apparently volunteered at some point to take on the major injuries, up to and including appendicitis, for our family.
The first time was my freshman year in college, when in chem lab I splashed potassium dichromate in my eye. The second was last Saturday.
I keep my kitchen knives sharp. I mean really sharp. They don't get put away without a touch-up honing. This is mostly a great thing, but let me just say that I take issue with the conventional wisdom that you're more likely to cut yourself with a dull knife than a sharp one. Brief encounters with a blade, which would never have broken the skin in my pre-knife-sharpening-obsession days, easily draw blood. They quickly heal and never hurt more than a paper cut, but it's annoying to try to keep the blood out of the vegetables. I mean, there goes any hope of getting approval by the Vegan Authorities.
Back to the story.
As I said, any cuts I get are almost always very minor. Almost. But even great chefs make the occasional mistake. Blame my new glasses, blame my distractable brain that had just received some nasty news on the financial front—but on Saturday when I was cutting up vegetables for a stew, just for a moment I lost the ability to distinguish between a carrot and my thumb.
I knew immediately that it wasn't serious, but neither was it a wrap-it-in-a-paper-towel-and-forget-it affair. I had made a nice, circular slice that very nearly lifted the top off my thumb. It was not deep, but "deep enough." I'm familiar with skin flap wounds, and know they don't tend to heal well on their own; mostly they dry up and fall off. I judged this to be a little too much for that to be desirable.
Wouldn't you know, Porter had moments before detailed to me his agenda for the afternoon. I wrapped up my thumb to staunch the blood, turned off the two stove burners where pans were cheerfully sizzling with the start of dinner, walked into his office and began, "I'm sorry to derail your afternoon plans, but...."
Let me just say this about my husband. He can get bizarrely upset about the littlest things, like a traffic light turning red, or a dice roll going against him in a board game. But give him a real emergency and he suddenly becomes calm, cool, and focussed.
Having had his own encounter with finger wounds, for which a doctor later admonished him, "You should have had stitches for this," he never questioned the need for emergency care. It didn't seem the right thing to go to our primary care doctor for, and there's no way I wanted to spend all day in a hospital emergency room after being subjected to a COVID test. Instead, he phoned our local doc-in-a-box CentraCare facility and (having been placed on hold) started driving. I have no idea where we were in the queue, because we were still on hold when we arrived and walked up to the receptionist.
Other than the phone call, I have to say that from beginning to end our treatment at CentraCare could not have been better. The waiting room was not crowded, and even so I jumped to the head of the line. Apparently blood, even when you've cleaned up and stopped the bleeding with a neatly-wrapped bandage before leaving home, gets people's attention.
The nurse (?) who attended me was great, and knew how to put me at ease. We had a great conversation because she's an EMT and studying to become a paramedic, and of course I had to talk about the EMT's and doctors in our family. Having determined that my wound did, indeed, need stitches, she then went off to inform the doctor.
Thus began the longest wait, which only makes sense because there was no longer an emergency. And I have no complaints, because when the doctor finally arrived, he gave me the (no doubt erroneous) impression that he had all the time in the world to attend to my needs. That's a precious gift, and rare from a doctor.
Turns out I didn't get stitches after all. After soaking my thumb in a "surgeon's soap" solution while he went to check on someone else, he told me that the cut was so neat that trying to stitch it would do more harm than good. (Did I mention that my knife was really sharp?) Instead, he just glued the flap in place with some specialized medical skin glue, and gave me a splint to wear.

That little device is brilliant. For one thing, it makes the wound look so much more impressive, and more worthy of having received medical attention. But mostly, it is great at keeping me from re-injuring the thumb. Without it there to protect against bumps and other stresses on the healing skin, and to remind me pay attendion, I would probably have re-opened the wound dozens of times in the course of daily life. The biggest frustration is not being able to get the thumb wet for seven days, which means I have to miss our water aerobics classes. And have you ever tried to wash just one hand? I have a friend whose neice was born with but one arm, and apparently has always managed beautifully. (When she was a small child, her younger sister was heard to exclaim, "I wish I only had one arm, so I could tie my shoes, too!") Let's just say I'm more impressed than ever. I also have a gut-level appreciation for what we were taught in high school biology class: the value of our opposable thumbs.
On Wednesday I went back to CentraCare to be told that everything is going great. (But I still can't get it wet till Saturday.) I made a point of telling them how impressed I was with their service, from the receptionist to the doctor and everyone in between.
That doesn't change the fact that I'm willing to wait another 50 years for my next visit.
P.S. Our initial stay was short enough that the food left on the stove was still safe when we returned home. Porter took over the cutting of the vegetables, and the stew was great.
Just yesterday I encountered the idea of how our primitive behavioral immune system fuels the bizarre fear, disgust, loathing, and anger that accompanies the COVID-19 vaccine debate, which I wrote about in my review of Norman Doidge's excellent article on the subject.
Today I ran headlong into a prime, and terrifying, example of just that, in a New York Times opinion piece by Paul Krugman, entitled "What to Do With Our Pandemic Anger." In my innocence, I assumed the article would be about the mental health crisis that has arisen from nearly two years of restrictions on normal human interaction.
I couldn't have been more wrong.
You may or may not be able to access the article—with the Times I find no rhyme nor reason as to when I can, and when I can't—so I'll quote a bit of it below and you can get the idea.
First, a reminder of what Doidge said about how the behavioral immune system [BIS] has hijacked our reason.
Many people’s mental set for the pandemic was formed early on, when the BIS was on fire, and they were schooled by a master narrative that promised there would only be one type of person who would not pose danger—the vaccinated person. Stuck in that mindset when confronted by unvaccinated people, about half of whom are immune, they respond with BIS-generated fear, hostility, and loathing. Some take it further, and seem almost addicted to being scared, or remain caught in a kind of post-traumatic lockdown nostalgia—demanding that all the previous protections go on indefinitely, never factoring in the costs, and triggering ever more distrust. Their minds are hijacked by a primal, archaic, cognitively rigid brain circuit, and will not rest until every last person is vaccinated. To some, it has started to seem like this is the mindset not only of a certain cohort of their fellow citizens, but of the government itself.
And now for a taste of what Krugman has to say.
A great majority of [New York City's] residents are vaccinated, and they generally follow rules about wearing masks in public spaces, showing proof of vaccination before dining indoors, and so on. In other words, New Yorkers have been behaving fairly responsibly by U.S. standards. Unfortunately, U.S. standards are pretty bad. America has done a very poor job of dealing with Covid. ... Why? Because so many Americans haven’t behaved responsibly. ...
I know I’m not alone in feeling angry about this irresponsibility.... There are surely many Americans feeling a simmering rage against the minority that has placed the rest of us at risk and degraded the quality of our nation’s life. There has been remarkably little polling on how Americans who are acting responsibly view those who aren’t ... but the available surveys suggest that during the Delta wave a majority of vaccinated Americans were frustrated or angry with the unvaccinated. I wouldn’t be surprised if those numbers grew under Omicron, so that Americans fed up with their compatriots who won’t do the right thing are now a silent majority. ...
I don’t claim any special expertise in the science, but there seems to be clear evidence that wearing masks in certain settings has helped limit the spread of the coronavirus. Vaccines also probably reduce spread, largely because the vaccinated are less likely to become infected, even though they can be. More crucially, failing to get vaccinated greatly increases your risk of becoming seriously ill, and hence placing stress on overburdened hospitals. ... You don’t have to have 100 percent faith in the experts to accept that flying without a mask or dining indoors while unvaccinated might well endanger other people—and for what? I know that some people in red America imagine that blue cities have become places of joyless tyranny, but the truth is that at this point New Yorkers with vaccine cards in their wallets and masks in their pockets can do pretty much whatever they want, at the cost of only slight inconvenience. ...
Those who refuse to take basic Covid precautions are, at best, being selfish—ignoring the welfare and comfort of their fellow citizens. At worst, they’re engaged in deliberate aggression—putting others at risk to make a point. And the fact that some of the people around us are deliberately putting others at risk takes its own psychological toll. Tell me that it doesn’t bother you when the person sitting across the aisle or standing behind you in the checkout line ostentatiously goes maskless or keeps his or her mask pulled down. ... Many Americans are angry at the bad behavior that has helped keep this pandemic going. This quiet rage of the responsible should be a political force to be reckoned with.
For someone who admits being no expert, Krugman is far from reluctant to make pronouncements based on questionable data. To his credit, he attempts to direct this "simmering rage" to political action, but the tone of the article is straight from, and speaks directly to, the behavioral immune system's primitive response of fear, disgust, and loathing. That cannot end well.
Believe it or not, I have left out the most vitriolic statements, which I deemed unnecessarily distracting.
Permalink | Read 1550 times | Comments (0)
Category Hurricanes and Such: [first] [previous] [next] [newest] Health: [first] [previous] [next] [newest] Politics: [first] [previous] [next] [newest] 95 by 65: [first] [previous] [next] [newest]
Are you tired of extremism and party politics surrounding talk about COVID-19 vaccination?
Me, too. I think you will love an article that recently came to my attention, and which is billed as,
... an attempt by a physician and neuroscience writer and someone who got vaccinated, early and voluntarily, to understand those who have not made this choice. This essay is not about COVID-deniers or anti-vaxxers, who oppose vaccines on ideological grounds. Nor is it about the activists or political figures who feed off and benefit from the corrosive discourse around vaccines. It is instead about the vaccine hesitant—those who are concerned and anxious about COVID but also anxious about these new vaccines. These are the people who are not yet vaccinated for reasons that the majority may not understand—and which are often more anchored in history and experience than the majority would suspect.
The article is called "Needle Points: Why so many are hesitant to get the COVID vaccine, and what we can do about it," by Norman Doidge. That link will take you to Part 1, from which you can click onward to Parts 2, 3, and 4. Or you can download a free, printable pdf of the whole thing. I found it fair, informative, and very important.
The only thing I know about Norman Doidge is that he wrote the fantastic book, The Brain that Changes Itself, which I read, reviewed, and loved back in 2010. I didn't even know he was the author of this article until after I'd read and appreciated it.
I have to warn you that it's a long article: 38 pages. It might be helpful to think of it as a very short book. I know many of my readers are turned off even by long quotation sections in my posts; how much more so by an article of this size? But it's worth it, really.
How do you eat an elephant?
I was hesitant to include quotations from the article, as it is an excellent whole that snippets cannot possibly do justice. But perhaps a few will whet some appetites.
Part 1 How vaccination is an approach to medicine that works with nature rather than seeking to conquer nature; How our primitive behavioral immune system contributes to the fear, disgust, and loathing that accompanies the vaccine debate; How the tyranny of the majority destroys democracy and impedes progress.
At times modern science and modern medicine seem based on a fantasy that imagines the role of medicine is to conquer nature, as though we can wage a war against all microbes with “antimicrobials” to create a world where we will no longer suffer from infectious disease. Vaccination is not based on that sterile vision but its opposite; it works with our educable immune system, which evolved millions of years ago to deal with the fact that we must always coexist with microbes; it helps us to use our own resources to protect ourselves. Doing so is in accord with the essential insight of Hippocrates, who understood that the major part of healing comes from within, that it is best to work with nature and not against it.
In humans (and other animals), any infection can trigger an archaic brain circuit in most of us called the behavioral immune system (BIS). It’s a circuit that is triggered when we sense we may be near a potential carrier of disease, causing disgust, fear, and avoidance. It is involuntary, and not easy to shut off once it’s been turned on.
The BIS is best understood in contrast to the regular immune system. The “regular immune system” consists of antibodies and T-cells and so on, and it evolved to protect us once a problematic microbe gets inside us. The BIS is different; it evolved to prevent us from getting infected in the first place, by making us hypersensitive to hygiene, hints of disease in other people, even signs that they are from another tribe.... We developed a system whereby anything or anyone that seems like it might bear significant illness can trigger an ancient brain circuit of fear, disgust, and avoidance. ... We see it firing every day now, when someone drives alone wearing a mask, or goes for a walk by themselves in an empty forest masked, or when someone—say with good health and no previous known adverse reactions to vaccines—hears that a vaccine can in one in 500,000 cases cause death, but can’t take any comfort that they have a 99.999% chance of it not happening because it potentially can. Before advanced brain areas are turned on and probabilities are factored in, the BIS is off and running. ... [It] is turned on in people on both sides of the debate. Those who favor vaccination are focused on the danger of the virus, and that triggers their system. Those who don’t are focused on the fact that the vaccines inject into them a virus or a virus surrogate or even a chemical they think may be poisonous, and that turns on their system. Thus both sides are firing alarms (including many false-positive alarms) that put them in a state of panic, fear, loathing, and disgust of the other.
[Alexis de Tocqueville noted that] in democracies, as long as there is not yet a majority opinion, a range of views can be expressed, and it appears there is a great “liberty of opinion,” to use his phrase. But once a majority opinion forms, it acquires a sudden social power, and it brings with it pressure to end dissent. A powerful new kind of censorship and coercion begins in everyday life (at work, school, choir, church, hospitals, in all institutions) as the majority turns on the minority, demanding it comply. Tocqueville, like James Madison, was concerned about this “the tyranny of the majority,” which he saw as the Achilles’ heel of democracy. It isn’t only because divisiveness created a minority faction steeped in lingering resentment; it’s also because minorities can sometimes be more right than majorities (indeed, emerging ideas are, by definition, minority ideas to start with). The majority overtaking the minority could mean stamping out thoughts and actions that would otherwise generate progress and forward movement.
Part 2 The long and complicated history of vaccination; How the National Childhood Vaccine Injury Act saved the vaccine supply while giving pharmaceutical companies incentives to take dangerous shortcuts with respect to vaccine safety; Stories of corruption, collusion, and deceit among government, academia, and pharmaceutical companies that could make any reasonable person begin to doubt everything that comes from public health authorities.
The kernel idea of exposing a person to a weakened form of a pathogen or toxin, known colloquially as “like to treat like,” long preceded modern medicine, and came in stages and through observation. ... The heal-harm paradox is a deep archetype in the human psyche. And it came not from Big Pharma but from everyday, often rural observations—one might even call them “frontline” observations about how nature works, and how the immune system behaves.
Because companies were indemnified [by the National Childhood Vaccine Injury Act] from any harm their vaccines might cause, they no longer had a powerful financial incentive to rectify existing safety problems, or even improve safety as time passed. Arguably, they were financially disincentivized from doing so. The solution shifted liability for the costs of safety problems from the makers onto the taxpayers, the pool that included those who were arguably harmed.
For a regular medication, a physician needs and has the ability to convince one patient at a time to take a particular drug. This is why pharmaceutical companies have huge marketing budgets to sway individual physicians and patients alike. In the case of vaccines, companies need to convince only a few key officials and committees, who then buy their product and market it for them to an entire population. For companies producing vaccines, mass marketing is replaced almost entirely by political lobbying.
The FDA bills Big Pharma $800 million a year, which in turn helps pay FDA salaries. Regulators also often get jobs in the pharmaceutical industry shortly after leaving the FDA or similar bodies; there is a huge incentive to impress, and certainly not to cross, a potential future employer. ...
This same compromised regulatory system allows Big Pharma to pay for, and play a key role in performing, the very studies that lead to the authorization of its own products. For decades, it was not just common for authors of studies to receive payments from the very companies making the medicines being tested; it was also systematically hidden. Drug companies secretly ghostwrote studies of their own drugs; Goldacre shows how they conscripted academics to pretend they had authored them. The papers were then submitted to mainstream journals, whose imprimatur would give the studies credibility, allowing these drugs to become the “standard of practice.”
In 2018, The New York Times’ pro-vaccine science writer, Melinda Wenner Moyer, noted with shock that she learned it was not uncommon among vaccine researchers to take the attitude that censoring bad news about their research was necessary.... "I’ve noticed that the cloud of fear surrounding vaccines is having another nefarious effect: It is eroding the integrity of vaccine science. ... When I tried to report on unexpected or controversial aspects of vaccine efficacy or safety, scientists often didn’t want to talk with me. When I did get them on the phone, a worrying theme emerged: Scientists are so terrified of the public’s vaccine hesitancy that they are censoring themselves, playing down undesirable findings and perhaps even avoiding undertaking studies that could show unwanted effects. Those who break these unwritten rules are criticized." ... If scientists play down their undesirable findings in potentially mandated medicines, as Moyer found them to be doing, they are not just missing opportunities for good science; they are potentially generating anti-scientific misinformation. “Vaccine scientists will earn a lot more public trust, and overcome a lot more unfounded fear, if they choose transparency over censorship,” she wrote.
As of a September 2019 Gallup poll, only a few months before the COVID-19 pandemic, Big Pharma was the least trusted of America’s 25 top industry sectors, No. 25 of 25. In the eyes of ordinary Americans, it had both the highest negatives and the lowest positives of all industries. At No. 24 was the federal government, and at No. 23 was the health care industry. ... At No. 22 was the advertising and public relations industry, which facilitates the work of the other three. Those inside the troika often characterize the vaccine hesitant as broadly fringe and paranoid. But there are plenty of industries and sectors that Americans do trust. Of the top 25 U.S. industry sectors .. only pharma, government, health care, and PR are seen as net negative: precisely the sectors involved in the rollout of the COVID vaccines. This set the conditions, in a way, for a perfect storm.
Part 3 This is by far the largest section of the paper (20 pages) and jam-packed with information on the debacle that was our response to the pandemic, from before the beginning ("gain of function" research) to shortly before the omicron variant appeared (the article was published in October 2021). No decent number of quotations can begin to do it justice. I'll put in a few; just be aware that there's so much more.
There were also disputes about lockdowns: Initially introduced as temporary to flatten the curve, they were later extended to become a new way of life, in order to save lives. But then some states like Florida, which didn’t impose long and severe lockdowns, had lower age-adjusted mortality than states like New York, which did. [emphasis mine]
Various observers argued that there was reason to consider that COVID may have leaked from the Wuhan Institute of Virology, and perhaps even may have been engineered by gain-of-function (GoF) research, in which a natural virus is made more contagious and lethal, ostensibly to see if the scientists can “get ahead” of nature, and to study how it operates in order to make new vaccines or medications, or for biological warfare. GoF is so controversial that in 2014 President Barack Obama put a moratorium on it. In 2017, Drs. Fauci and Francis Collins, then director of the NIH, who had opposed the moratorium, succeeded in having it lifted. But Fauci asserted that the scientists who were in a position to judge the COVID situation concluded that its origin was natural. The media followed suit, and called those who thought otherwise “conspiracy theorists.”
If you asked researchers or most physicians in the spring of 2020 how long it normally takes to produce a vaccine safe enough to administer to patients, many would have pointed out that the average fast vaccine takes 7-10 years, and that the first vaccine might just be one of several required to end a given crisis—because often the first is not the best.
Indemnification for vaccines was, as discussed above, not unique; what was new was that the companies producing them were indemnified before the vaccine was even made and fully assessed—knowing it would all be done faster than ever before.
AstraZeneca, Pfizer, and Moderna had each withheld their study protocols from outside scientists and the public. Withholding protocols guarantees that outside researchers can’t know how participants are selected or monitored, and how effectiveness or safety are defined, so they can’t really know what exactly is being studied. ... This is part of a kind of “traditional secrecy” in the field. Delaying protocol release conveniently means that it is a company’s press releases, not the verified science, that dominate the public’s all-important initial impression of its product. ... That the government’s regulatory agencies go along with all this—it is, in fact, standard practice—doesn’t assuage the public; for many, it makes the whole process appear corrupt. ...
The essence of the scientific method is conducting experiments that everyone can objectively see and verify; transparency is the bedrock of experimental science, and the means to ultimately dispel doubt. Moreover, in terms of the scale of public involvement, the experience of the summer and fall of 2020 was unlike any other in the history of medicine. Never before had studies of this size and consequence been run so quickly, or a medicine been produced so quickly to be given to hundreds of millions of people. ... How long were the patients followed ... after their second dose, to assess safety and efficacy? Two months. On that basis the vaccines were given to over a hundred million people. [emphasis mine]
What we shouldn’t do, if we want to maintain public trust and cohesion, is act as though there is no chance that any legitimate concern could ever possibly emerge, or that we know more than we really do after only two months of study. With complex biological systems, we simply can’t presume that just because we have a fantastic idea for a treatment, the safety we hope for and see at the start will necessarily hold over time.
“Efficacious” is the term used to describe how effective a treatment is in the artificial situation of a clinical trial with volunteer patients, a group not always representative of the wider population; “effective” is the term used to describe how a treatment works in the real world. The media quickly assumed the two were the same. To them, hearing that a vaccine was “95% efficacious” meant it was practically perfect, which the press repeated over and over.
After the protocols were released, Peter Doshi, an associate editor at the British Medical Journal who does research into drug approval processes and how results are communicated to the public, tried to sound an alarm: “None of the trials currently underway are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths,” he said. Only one of the studies, of the Oxford AstraZeneca, looked at whether vaccinated individuals were less likely to transmit virus.... So what were these clinical trial studies that showed 95% and 94% efficacy looking at, if not saving lives and viral transmission?
Though it would fall to the FDA to officially approve the vaccines, the advice to enact vaccine mandates would come from a small network, and would be based on studies that were authored in some instances by people who are employees of the companies themselves, which were testing their own products. And when a remarkably trusting public and a few scientists requested a look at the raw data, they got stiffed.
One can only imagine how enriched our knowledge would be if it were otherwise—if, to take just one example, the raw data were available and verified by the hive mind of world scientists, who, drilling down, could see for whom the vaccine was most effective, and who was most at risk of serious side effects, in order to follow them longer than two months and to protect those groups of people in the future.
In April, during a White House press briefing barely four months after distribution of the first vaccine doses began, Walensky announced that the “CDC recommends that pregnant people receive the COVID-19 vaccine.” But if you checked the CDC website that day—as many pregnant women and their physicians of course did—you would have found something different: “If you are pregnant, you may choose to receive a COVID-19 vaccine,” but “there are currently limited data on the safety of COVID-19 vaccines in pregnant people.”
The mainstream media in the United States also often downplayed potential problems, and even demonized those who took them seriously—portraying white Christian Republicans as the last redoubt of COVID vaccine skepticism in America. But if white Americans in red states have had high rates of hesitancy, African Americans and Latinos have too. As we’ve seen in the case of African Americans, hesitancy is based at least in part on well-earned distrust. In the U.K., in March 2021, vaccination rates were very high in the “white British” group (91.3%), and British Christians had the least hesitancy, whereas vaccination rates were lower in the Black African and Black Caribbean communities (58.8% and 68.7% respectively), and among Muslims, Buddhists, Sikhs, and Hindus. ...
Given the WHO’s own definition of the “vaccine hesitant”—people who delay or are reluctant to take a vaccine—one could say that 52% of frontline U.S. health care workers were vaccine hesitant at the beginning of the year. It was hard to argue that these were people who got all their information from a few rancid conspiracy websites. ...
We are told that the hesitant are only those with the least education. But a Carnegie-Mellon and University of Pittsburgh study showed that “by May [2021] PhDs were the most hesitant group.”
On June 3, three scientists from an FDA advisory committee—Dr. Aaron Kesselheim, professor of medicine at Harvard Medical School, Joel Perlmutter, M.D., a neurologist at Washington University in St. Louis, and David Knopman, M.D., a neurologist at the Mayo Clinic—resigned because of the way an Alzheimer’s drug, Aduhelm, was approved. In a letter, Kesselheim claimed that the authorization of Aduhelm—a monthly intravenous infusion that Biogen has priced at $56,000 per year, which some worry could bankrupt Medicare—was wrong “because of so many different factors, starting from the fact that there’s no good evidence that the drug works,” that it was “probably the worst drug approval decision in recent U.S. history,” and that this “debacle … highlights problems” with the FDA advisory committee relationship.
The Pfizer study [of booster shots] was surprisingly tiny: Only 306 people were given the booster. As vaccine researcher David Wiseman (who did trials for rival Johnson & Johnson) pointed out at the FDA meeting, “there was no randomized control” in the Pfizer study. The subjects were younger (18-55) than the people who are most at risk of COVID death or serious illness, and were followed only for a month, so we didn’t actually know how long the booster would last, or if adverse events might show up after the 30 days. They were not followed clinically, so there was no information on infections, hospitalizations, or deaths. ... The study was too small, and the FDA panel held two votes on approval. In the first, it voted overwhelmingly (16 to 2) against approving Pfizer boosters for all ages; in the second vote, the panel supported boosters only for people over 65 or special at-risk groups. And yet, in mid-August, Biden began publicly supporting boosters for all.
Along with the widespread attacks on scientists who had criticisms of the simplified master narrative (including ones from major universities like Harvard, Yale, Stanford, Rockefeller, Oxford, and UCLA), many average Americans learned that certain major stories weren’t as widely known as they might have been, thanks in part to censorship by Big Tech. In May, Facebook announced that it would no longer censor stories about the lab leak theory, which was how many people found out that it was in fact a viable scientific theory in the first place. (Facebook’s idea of transparency is telling you when it’s stopped censoring something; the same goes for YouTube.)
Meanwhile, three U.S. medical boards—the American Board of Family Medicine, the American Board of Internal Medicine, and the American Board of Pediatrics—went beyond censorship by threatening to revoke licenses from physicians who question the current but shifting line of COVID thinking and protocols. This forced doctors who had any doubts about the master narrative to choose between their patients and their livelihoods.
Things got so bad globally that Amnesty International eventually issued a report on this crisis: “Across the world, journalists, political activists, medical professionals, whistle-blowers and human rights defenders who expressed critical opinions of their governments’ response to the crisis have been censored, harassed, attacked and criminalized,” it noted. The typical tactic, the report’s authors say, is “Target one, intimidate a thousand,” whereby censors justify these actions as simply banning “misinformation” and “prevent[ing] panic.” The report goes on: “Evidence has shown that harsh measures to suppress the free flow of information, such as censorship or the criminalization of ‘fake news,’ can lead to increased mistrust in the authorities, promote space for conspiracy theories to grow, and the suppression of legitimate debate and concerns.”
Science, as the Nobel Prize winning physicist Richard Feynman pointed out, requires questioning assertions: "Learn from science that you must doubt the experts … When someone says science teaches such and such, he is using the word incorrectly. Science doesn’t teach it; experience teaches it. If they say to you science has shown such and such, you might ask, “How does science show it—how did the scientists find out—how, what, where?” Not science has shown, but this experiment, this effect, has shown. And you have as much right as anyone else, upon hearing about the experiments (but we must listen to all the evidence), to judge whether a reusable conclusion has been arrived at."
Note how emphatic Feynman is that it’s not just the few who conduct the experiments, or even just “the experts,” who have a right to discuss and judge the matter. This is especially true in public health, because the field is so broad and composed of many disciplines, from those that deal narrowly with viruses to those that deal with mass behavioral changes.
When public health and allied medical and educational organizations censor scientists and health care professionals for debating scientific controversies—thus giving the public the false impression that there are no legitimate controversies—they misrepresent and grievously harm science, medicine, and the public by removing the only justification public health has for asking citizens to undergo various privations: that these requests are based on a full, unhampered, and open scientific process. Those who censor or block this process undermine their own claim to speak in the name of science, or public safety. [emphasis mine]
If we didn’t get to have a properly open scientific process, what did we get instead? Government enmeshment with legally indemnified corporations, public health officials misleading Congress, multiple honest regulators leaving the FDA because of inappropriate approvals, FDA heads taking Big Pharma jobs directly related to products they had just been involved in approving, a possible lab leak that couldn’t be discussed as such for more than a year so that it couldn’t be clearly disconfirmed, faceless social media platforms admitting that they control what we see and don’t see, and institutional censorship of many kinds.
Throughout the pandemic, Israel had extensive lockdowns. In contrast, Sweden became famous for never having locked down. Israel and Sweden have about the same size population (9 million and 10 million, respectively), and have almost identical rates of double-vaccinated people, if you take in all ages including children (63% Israel, 67% Sweden). If anything, Israel has the edge over Sweden because 43% of Israelis are also triple vaccinated. Yet the difference in the number of hospitalized patients is staggering. For the week of Sept. 12, 2021, Israel had 1,386 COVID hospitalizations, which was four times that of Sweden (340). Israel had a rolling seven-day average of 2.89 deaths per million, compared to the much lower number of deaths in Sweden (0.15).
What can account for this? Many argue that because Sweden (where public health works on a voluntary, participatory basis) never locked down, many more people there were exposed and got natural immunity. The Swedes had hoped to protect the most vulnerable in nursing homes, which they failed to do because of poorly trained staff—but in this they were no different from most Western nations that did lock down. Sweden also suffered more deaths per 100,000 than Israel overall. But through the summer of 2021 Sweden dropped to about 1.5 deaths a day from COVID. Its hospitals were never overwhelmed, suggesting that, once Sweden’s natural herd immunity was established, combined with its vaccines, it was now more protective than Israel’s largely vaccine-based immunity.
This wasn’t what the master narrative had promised.
The FDA had originally said that a vaccine less than 50% effective (defined as reducing the risk of having to see a doctor) would not be approved by regulators. Now something that appeared to the public to be significantly less effective was being not just approved but mandated. [emphasis mine]
U.S. government officials and the media chose to assert, soon on a daily basis, that the country was now in “a pandemic of the unvaccinated,” even though it was now clear that the vaccinated could get infected and transmit the virus. ...
Headlines about waning vaccines expressed despair that this pandemic might never end. ... Instead of addressing how this disappointment might affect people, U.S. public health talking heads and Twitter-certified human nature experts turned now to behavioral psychology, a very American form of psychology, to deal with the crisis—treating their fellow citizens like children or lab rats to be given rewards when “good” and punishments when “bad.” Some seemed to relish telling people that if they didn’t just do what the experts told them to do, they’d lose their jobs, their place in school, or some other basic need, like mobility.
On Aug. 23, FDA approval of the Pfizer vaccine came through. It was based on the same patients who were in the study that previously included only two months of follow-up, but which now had six months of follow-up. With the approval, Pfizer officially stopped the randomized control trials and informed the controls they never got the vaccine. Now that they know they are not vaccinated, the controls may well choose (or be mandated) to get vaccinated, so we won’t be able to follow them as a control group any more. That means the only randomized control trials we have of these vaccines are just six months long. Should some independent party—not a drug company—want to do a new RCT of the vaccine, they will find it almost impossible to do so, because it will be hard if not impossible to find people who were not vaccinated, or not already exposed to COVID. ... This is especially important because we don’t yet—we can’t yet—have any good randomized control trial data to rule out long-term effects. [emphasis mine] ...
We could use good studies comparing the COVID-induced myocarditis rates and vaccine-induced myocarditis rates by age and sex. Which is why it’s so unfortunate that the RCTs were not much larger, and that they didn’t go on longer. Had they continued, and if their data ever became transparent, it could really help us in assessing long-term safety in a more reassuring way—that’s what RCTs are good at. One can more persuasively demonstrate that a vaccine doesn’t have these effects if there is a proper vaccine-free, COVID-free control group. But if vaccines continue to be pushed as the one and only answer, we will never know if certain health problems emerge, because there will be no “normal” vaccine-free group left for comparison. It’s a development that is quite disconcerting, for it suggests a wish not to know.
When the pandemic first broke, many were certain that the developing countries—with their inability to afford vaccines, malnutrition, crowded cities, and lower numbers of health care workers—would be universally devastated. But that prediction turned out not to be true. The population of Ethiopia is about 119 million—just over one-third of the United States. COVID vaccination rates are very low there: 2.7% have had at least one shot, 0.9% have had two. As of Sept. 28, 2021, the country recorded only 5,439 COVID deaths over the course of the entire pandemic. If the United States had such a death rate per capita, it would have lost just over 16,000 people, rather than over 700,000.
The very fact that we frame the threat debate between the “vaccinated” and the “unvaccinated” has always been peculiar; some epidemiologists point out that the categories we should be thinking of instead are the “immune” and those who are “not immune.” The European Union has a Digital Covid Certificate, which is not limited to proof of vaccination. You can get one and travel if you have been vaccinated or if you have “recovered from COVID-19.” This allows travel among all EU member states. American officials always proclaim they are “following the science,” but obviously, if the science gave clear orders, then European scientists would have received them too.
Vaccination is a tool, a means to an end: immunity. But the American government has made the means, vaccination, the new end. This strange substitution, or reversal, reveals the master narrative to be the expression not of science, but of a new kind of scientistic ideology, which we might call “vaccinism.” But vaccinism is not a treatment; it’s a mindset, one that takes a wonderful invention—which, if used properly and carefully, can be outstandingly productive—and makes it the only tool worth having, until it becomes, at times, counterproductive. It makes no exceptions; indeed, it is insulted by the idea of any exemptions. In its all-or-nothing approach, it is the ideological mirror of anti-vaxxism. [emphasis mine]
Part 4 Returning to the concept of the behavioral immune system (BIS); Why herd immunity through vaccination is not an achievable goal with this virus; The critical importance of natural immunity (i.e. getting COVID and recovering from it); The disastrous consequences of vaccine mandates and vaccine passports; and Some ideas for restoring trust in our public health system.
Many people’s mental set for the pandemic was formed early on, when the BIS was on fire, and they were schooled by a master narrative that promised there would only be one type of person who would not pose danger—the vaccinated person. Stuck in that mindset when confronted by unvaccinated people, about half of whom are immune, they respond with BIS-generated fear, hostility, and loathing. Some take it further, and seem almost addicted to being scared, or remain caught in a kind of post-traumatic lockdown nostalgia—demanding that all the previous protections go on indefinitely, never factoring in the costs, and triggering ever more distrust. Their minds are hijacked by a primal, archaic, cognitively rigid brain circuit, and will not rest until every last person is vaccinated. To some, it has started to seem like this is the mindset not only of a certain cohort of their fellow citizens, but of the government itself.
For many, trust was broken by the lockdowns, which devastated small businesses and their employees, even when they complied with safety rules, such that an estimated one-third of these businesses that were open in January of 2020 were closed in April of 2021, even as we kept open huge corporate box stores, where people crowded together. These policies were arguably the biggest assault on the working classes—many of whom protected the rest of us by keeping society going in the worst of the pandemic—in decades. That these policies also enriched the already incredibly wealthy (the combined wealth of the world’s 10 richest men—the likes of Jeff Bezos, Mark Zuckerberg, Bill Gates, and Larry Page—is estimated to have risen by $540 billion in the first 10 months of the pandemic), and that various politicians who instituted lockdowns were regularly caught skirting their own regulations, solidified this distrust.
And yet, it is the unvaccinated whom many leading officials still portray as recklessly endangering the rest of the country. “We’re going to protect vaccinated workers from unvaccinated coworkers,” President Biden has said. The unvaccinated are now presented as the sole source of future variants, prolonging the pain for the rest of us. For those in favor of mandates, the vaccine is the only way out of this crisis. To them, the vaccine hesitant are merely ignorant, and defy science. We tried to use a voluntary approach, they believe, but these people are Neanderthals who must now be coerced into treatment, or be punished. Among the punishments called for is not just loss of employment, but also of unemployment insurance, health care, access to ICU beds, even the ability to go to grocery stores.
So, if it’s correct that we can’t eradicate the virus, and we can’t get a lasting vaccine-induced herd immunity, what is our goal? It would be, to use Monica Gandhi’s phrase, “to get back to normal.” It would mean accepting some natural herd immunity and putting more focus on saving lives by other means alongside vaccines—including better outpatient medications to catch COVID early and keep people out of the hospital; lowering our individual risk factors; and speeding delivery of vaccines to the highly vulnerable when an outbreak occurs, and prioritizing them over people who are already immune.
“Right now with these vaccine mandates, and vaccine passports, this coercive thing is turning a lot of people away from vaccines, and not trusting them for very understandable reasons,” [says Harvard’s Martin Kulldorf, a leading epidemiologist and expert in vaccine safety]. “Those who are pushing these vaccine mandates and vaccine passports—vaccine fanatics I would call them—to me they have done much more damage during this one year than the anti-vaxxers have done in two decades. [emphasis mine] ...
In tackling the trust problem generally, we can return to the two kinds of public health systems, the coercive and the participatory. The United States has all sorts of mandates, but also continues to have significantly high rates of vaccine hesitancy and vaccine avoidance. In contrast, Sweden is the leading example of a participatory public health model. “Sweden has one of the highest vaccination rates in the world, and the highest confidence in vaccines in the world. But there’s absolutely no mandate,” Kulldorff notes. “If you want to have high confidence in vaccines, it has to be voluntary.... If you force something on people, if you coerce somebody to do something, that can backfire. Public health has to be based on trust. If public health officials want the public to trust them, public health officials also have to trust the public.” Just as pharma’s indemnification removed its incentive to improve safety, so do mandates remove public health’s incentive to have better, more consistent communication—to listen, understand, educate, and persuade—which is what builds trust.
And finally, let's return, as the author does, to Alexis de Tocqueville, and a quotation I'm certain I will pull out in other contexts:
Protection, therefore, against the tyranny of the magistrate is not enough: there needs protection also against the tyranny of the prevailing opinion and feeling; against the tendency of society to impose, by other means than civil penalties, its own ideas and practices as rules of conduct on those who dissent from them; to fetter the development, and, if possible, prevent the formation, of any individuality not in harmony with its ways, and compel all characters to fashion themselves upon the model of its own. There is a limit to the legitimate interference of collective opinion with individual independence: and to find that limit, and maintain it against encroachment, is as indispensable to a good condition of human affairs, as protection against political despotism.
As usual, that was more than "a few" snippets from the article. I hope they encourage you to read the whole thing, rather than giving you the impression you know all that's important in it. It is the clearest, most comprehensive, and most reasonable explanation I have yet encountered for what has been happening to the world in the last two years. Once again, here's the article link.
Our city has long been in the forefront of innovation when it comes to wastewater treatment. I'm proud of Altamonte Springs. The latest news, however, has me puzzled.
They're now testing our wastewater for evidence of COVID-19 infections.
Actually, I think that sounds clever. It's the results I question. According to this news story, 70% percent of our residents are infected with COVID-19.
Seventy percent! Does that make any sense at all? Later in the same story, it is claimed that half of the people getting tested are positive.
Wait just a minute. Who is it who gets tested? I know that some folks submit to testing, sick or not, because of their jobs, their travel plans, or because they've gone into the hospital with a broken leg and been tested for COVID because that's what hospitals do. But generally speaking, the people who bother to get tested are those who are experiencing some symptoms of illness. Those of us who think we are healthy don't bother.
So how is it that 70% of us actually have COVID when the tests, heavily weighted towards those who know they are sick, are only coming in at 50%?
All I can think of is that the COVID tests, or being ill with something other than COVID, or even breaking your leg, is somehow protective against the COVID-19 virus itself.
This may be a strange disease, but come on, it's not that strange.
I thought I'd already published my New Year's Eve post, but this heartbreaking news from Quebec demands publicity. For those who don't want to watch the 11-minute video, I've put a short summary afterwards.
Quebec has been iron-fisted from the beginning in its reaction to COVID-19, with tight lockdowns, cancellations, closures, severe restrictions on gatherings in private homes, travel bans, strong vaccine-passport requirements, and even a harsh, five-month curfew.
After much suffering on the part of the Quebec citizenry, the curfew was lifted and the choke-hold on the province's economy and family life began to ease, just a little. Enough for people and businesses to start making plans again.
Until yesterday.
That's when the provincial government announced new extrememe measures in the light of Omicron, the newest COVID variant. These include
- reinstated curfew
- take-out only for restaurants
- no private gatherings in your own home
- in-person school shut down at least until mid-January
And when do these measures take effect? At 5 p.m. today.
Today. New Year's Eve.
Now, I'm not one to go crazy on New Year's Eve. This image I found on Facebook sums it up pretty well for us these days.
But I realize that for many people the New Year's Eve festivities are important. They make plans, they travel, they spend lots of money on clothes and event tickets and parties and food and special restaurant meals. Restaurants, event venues, musicians, caterers and loads of other businesses count on this time to keep them financially afloat.
The decree comes out with one day's notice, and is clearly calculated to pull the rug right out from all New Year's Eve festivities. Plans are already made, tickets purchased, food bought, extra help hired ... then nothing. And all in fear of a COVID variant that has been producing high numbers but is almost always a mild illness with very low hospitalization and death rates.
This is not just tyrannical. It is sadistic.
I wouldn't go so far as to call it Fascist. But it is certainly Faucist.*
We cannot continue to ignore the economic, social, and mental health consequences of these extreme measures.
(Sorry this post is so depressing. My first post of the new year will be more delightful and uplifting.)
*Porter gets credit for this term, but I've latched onto it enthusiastically.
Those who are smart and protecting themselves need to continue doing their best to protect themselves and their loved ones.
I found this in a comment on a friend's Facebook post. One advantage of information overload is that such comments quickly become "anonymized information" in my brain, protecting the innocent and the guilty alike.
What struck me about this statement, with which I heartily agree, is what it tells me about how much we are alike. We all want to protect ourselves and our loved ones, and most of us have opinions as to how best to do that.
It is in the means, not the ends, that we disagree.
Some people move to rural areas and learn to farm. Some organize and join unions. Some purchase and learn to use guns. Others choose to homeschool, or to take political action, or to stockpile food and other essentials. Some work hard to strengthen family and community ties, or to attend to their own physical fitness, or to build up a strong financial base. And some people get vaccinated against COVID-19. Many choose more than one of these paths.
The writer of the Facebook comment was specifically speaking of COVID-19 vaccination, which I certainly consider to be a valid way of choosing to protect oneself and one's family. Unfortunately, the context of the above quotation wasn't as reasonable.
I know this is callous, but those who are smart and protecting themselves need to continue doing their best to protect themselves and their loved ones. What happens to those who do not care, is no longer taking up my headspace.
Just as the excerpt epitomizes what we have in common, the context shows what is dividing us. Because by "those who do not care," the writer appears to mean those who choose not to follow his own particular choices. Possibly, he's expressing his willingness to leave them alone to make their own decisions. But the callousness, which he admits, contains the implication that he considers doing them harm to be a valid part of protecting himself.
That is very dangerous ground indeed. We can do better.
Permalink | Read 1147 times | Comments (0)
Category Hurricanes and Such: [first] [previous] [next] [newest] Health: [first] [previous] [next] [newest] Politics: [first] [previous] [next] [newest] Random Musings: [first] [previous] [next] [newest]
"Find Your ZZZs: How to Get the Best Sleep Every Night"
It was a two-page article in our local city newspaper—and very large print at that. So I certainly couldn't have expected anything profound. I'm only calling it out because I was struck by how inapplicable it was to me. The advice given must work for many people, because I've heard it in just about every article I've read about sleep. But one size simply doesn't fit all, and I wish that were more universally acknowledged. Here's some of the advice given:
- Set your bedtime so that you wake up at the end of a 90-minute sleep cycle Not applicable, since I'm one of the blessed people who almost never uses an alarm clock. I wake up when I wake up, and figure there's no need to worry about sleep cycles.
- 30 minutes to an hour before bedtime, turn off bright lights and put devices away "Avoiding screen time at least 30 minutes before bed is critical to your quality of sleep." That's a very common recommendation, but for me just a few minutes of reading or doing puzzles in bed is the best trick I've found for putting me right to sleep, and it doesn't matter a bit whether they're print or electronic.
- Decrease the amount of disruptive light in the room with blackout curtains or a sleep mask. This might actually be useful. Light doesn't keep me from falling asleep, but our neighbor's bright, motion-activated light does wake me up and make me wonder which of our wild animals is dancing on the lawn.
- Keep your room a cool temperature (experts suggest between 60 and 67 degrees) Right. Maybe that works for a northerner, but running the A/C that much is not in our budget. Besides, at that temperature, I'd be wearing my winter pajamas and huddling under the blankets.
- Invest in your sleep with a supportive bed and comfortable bedding You mean the mattress and box springs we got second-hand from my in-laws almost 20 years ago should be replaced? At least the author had the grace to admit that "upfront costs of a new bed may be intimidating"—as we re-discover every time we think we might do just that.
- Don't use the snooze button Not a problem, since I'm not using an alarm clock.
- Expose yourself to sunlight when you get up Hmm. I think not. Since I'm usually up a couple of hours before sunrise, that's not going to happen; it's especially hard during Daylight Saving Time.
I'm not complaining; I'm sure the article was helpful for some folks. But I do find that more and more these days people are over-generalizing when it comes to what other people are like. I guess we just need to be more aware of what truly works for us and not worry about what other people think.
Actually, I do have one complaint, I suppose: With all that advice about going to bed and waking up, they did not address the only trouble I do have with sleeping: getting back to sleep after awakening in the middle of the night! Praying is the best help with that—but only memorized prayers; if I have to think to any extent it only speeds the squirrel-wheel in my brain.
In research inspired by my previous post, Measles Wipes Out the Immune System?, I discovered this interesting article on another disease, polio. Most of all I was struck by this explanation of the huge spike in the disease that occurred in the middle of the 20th century:
Up to the 19th century, populations experienced only relatively small [polio] outbreaks. This changed around the beginning of the 20th century. Major epidemics occurred in Norway and Sweden around 1905 and later also in the United States. Why did we see such large outbreaks of polio only in the 20th century?
The answer ... lies with hygiene standards. As polio is transmitted via the fecal-oral route, the lack of flush toilets and the lack of safe drinking water meant that children in the past were usually exposed to the poliovirus before their first birthday already. At such a young age, children still benefit from a passive immunity that is passed on from their mothers in the form of antibodies. ... Thereby, virtually all children would contract the poliovirus at a very young age. While protected from developing the disease thanks to the maternal antibodies, their bodies would produce their own memory cells in response to the virus and that ensured long-term immunity against polio. The latter is important as the mother’s cells have a half-life of only 30 days (starting from the last day of breastfeeding). Once the maternal antibodies decrease in number, children lose their passive immunity. As hygiene standards improved, the age at which children were first exposed to the poliovirus increased and this meant that the maternal antibodies were no longer present to protect children from polio.
That improved sanitation was a driving factor in polio outbreaks is also illustrated by the fact that the age at which polio was contracted increased over time. During five US epidemics in the time period 1907-1912, most reported cases occurred in one- to five-year-olds, whereas during the 1950s the average age of contraction was 6 years with "a substantial proportion of cases occurring among teenagers and young adults." Being exposed to the poliovirus after losing the protection from maternal antibodies meant that they were more likely to get polio.
The dramatic dropoff in cases in the 1950's shows the effectiveness of the newly-developed polio vaccine.
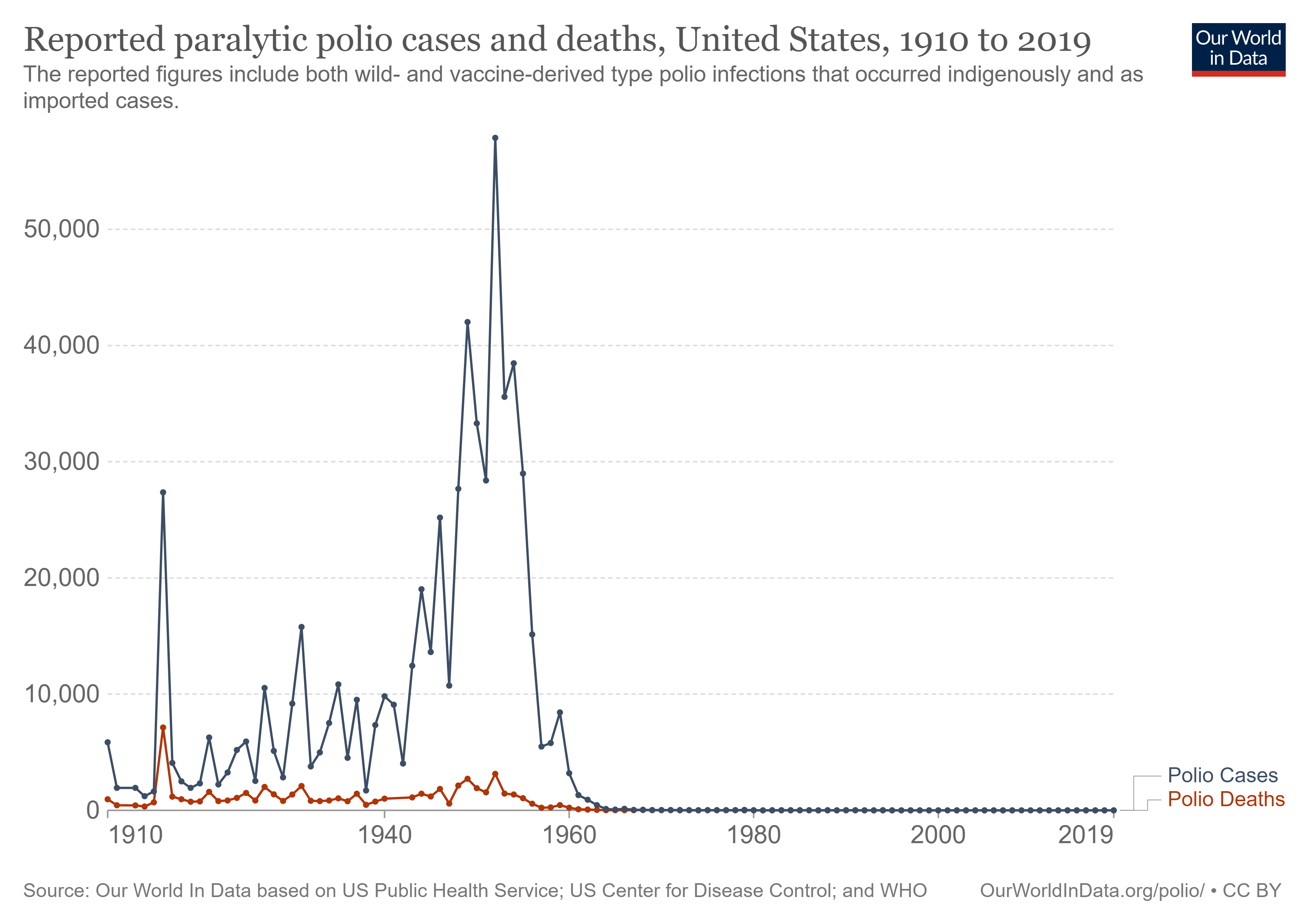
I find the progression fascinating. The world achieves a steady-state coexistence with the disease, in which mothers' acquired immunity protects their children while the children develop immunity of their own. Then, thanks in large part to laudable and desirable public health advances, the disease gets the upper hand and skyrockets. (The article does not mention this, but I'm certain that the decline of breastfeeding during this time period also contributed significantly to the disruption of the natural protection against polio.) Finally, vaccine development and widespread implementation nearly wipes out the disease.
The emphasis on "nearly" is important. There is hope that, like smallpox, polio will completely eradicated. Smallpox dropped off the list of recommended vaccines when the risk from the vaccine became greater than the risk of the disease. Someday soon I hope the polio vaccine will also be relegated to history. In the meantime, however, we must not become careless nor complacent about the vaccine. We no longer have the natural immunity passed between mothers and children, and nothing short of a catastrophe will return us to those times. We have reason to feel quite safe here in the United States, but consider this from the article:
As of 2017 the virus remains in circulation in only three countries in the world—Afghanistan, Pakistan and Nigeria.
Do we want to completely shut our doors to the visitors, immigrants, and refugees who come here from these countries? If not, we'd better continue to make vaccination against polio a priority.
Here's a very strange news story out of the usually-reasonably-trustworthy BBC News: Measles resets the immune system.
"Immune amnesia" [is] a mysterious phenomenon that's been with us for millennia, though it was only discovered in 2012. Essentially, when you're infected with measles, your immune system abruptly forgets every pathogen it's ever encountered before—every cold, every bout of flu, every exposure to bacteria or viruses in the environment, every vaccination. The loss is near-total and permanent. Once the measles infection is over, current evidence suggests that your body has to re-learn what's good and what's bad almost from scratch.
Scientists have known for decades that even after they recover, children who have been infected with measles are significantly more likely to fall ill and die from other causes. In fact, a study from 1995 found that vaccinating against the virus reduces the overall likelihood of death by between 30% and 86% in the years afterwards.
I find this bizarre and completely counter-intuitive. Nearly everyone my age and older has experienced a measles infection, and this phenomenon doesn't make sense given my experience and that of those I know, i.e. that of normal, healthy, well-nourished children who have suffered from measles. I say "suffered," but will make the point that in my case it was hardly suffering. Measles was just one of several infections that got you out of school for a week or two and earned you extra parental attention and breakfast in bed.
What we were not is sickly. We were nothing if not robust. Polio had been licked by the new vaccine, and everything else we endured for a few days and then were back in the business of causing general havoc in the fresh air and sunshine.
Probably the greatest threat to our health was secondhand smoke: nearly everyone smoked nearly everywhere. That and the strontium-90 cloud that passed through our village in my early childhood....
If our immune responses had been wiped out by getting measles, I would think we'd have seen an increase in illnesses post- versus pre-measles. Does anyone of my generation remember that? I don't. If our immune systems forgot every other vaccine and pathogen they had previously encountered, they seem to have re-learned their responses quite quickly.
Certainly the subsequent generations of children do not seem to me to be noticeably healthier than my own, if you consider the "normal, healthy, well-nourished" cohort I mentioned above. New vaccines have kept them free of most of the early childhood diseases, but instead of dealing with a few days of illness they're at increased risk of lifelong asthma, any number of food allergies, and even autism. Correlation does not imply causation—but let's just say that I don't feel I got a bum deal growing up in the 1950's. Except for the secondhand smoke part.
I'd like to hear more about this new discovery of the effects of measles. Crazier things are true. It just seems weird to me.
As I wrote before, we recently made our first airplane voyage since before the start of the pandemic. I was surprised at how rusty we were in what used to be accustomed procedure!
Overall, I was impressed, as I usually am, by Southwest Airlines. We flew during their recent—and never satisfactorily explained—outage, and our outbound flights were cancelled. However, we were automatically rebooked, within minutes of that notification, on a flight that left later the same day and arrived at our destination earlier, a much better situation for us. Between that and having automatic TSA Precheck, our airport experiences were problem-free. And I'm very happy about the improved cleaning and air filtration procedures, since in my experience an airplane is nearly as dangerous as an elementary school when it comes to challenges to the immune system. That part of the flight felt good.
Not that we had all that much chance to experience the new, fresher air, as masks were required to be worn at all times, even between bites and sips while eating and drinking. Fortunately, the between bites part was not aggressively enforced, but neither was there all that much opportunity for eating and drinking.
I can handle a mask, when necessary, for short shopping trips, and can make it through a choir rehearsal or a church service, albeit with difficulty. If I had to wear a mask for my job, I'd be applying for a medical exemption. I have no disability other than age, but that was good enough to get me priority for the vaccine, so maybe it would work. Fortunately, employment is not an issue.
Wearing a mask for the trip was hard. Ours was a relatively short flight, but that was three hours, and of course you have to add in the airport time on either end. Still, we managed all right, as far as I could tell.
The scary part was on the flight home, when I had the elbow room to use the sensor on my phone to check my blood oxygen. I know I'm good at sleeping on airplanes, but I couldn't stay awake to read a very interesting novel, and that concerned me. The sensor on my phone is hardly as accurate as a medical pulse oximeter, but there has to be something wrong about the fact that it consistently reads between 95% and 100% at home (usually on the high side of that), and my readings on the plane were between 84% and 90%! Pulling the mask away from my face for several breaths got it up to between 93% and 97%. But for how long had I been in the danger zone? Was the problem due to wearing the mask, or the altitude, or a combination? All I know is that when I got back home the numbers were up to 97%-100% again.
I'm trying not to think too much about the fact that our overseas family, including small children, had to endure two very long transatlantic flights for their Christmas visit here, and were forced to wear medical masks because their own cloth masks—similar to mine—were deemed to allow too much air exchange.
This won't stop me from flying again, even overseas when that is allowed. Family is too important. But at my age I need all the brain cells I can keep. Who doesn't, at any age? (That's one reason I avoid anesthesia whenever possible.) I'm more and more convinced that the harmful effects of our pandemic regulations are only just beginning to be felt.
My constant prayer since the start of the development of the COVID-19 vaccines has been that the knowledge gained would lead to an effective vaccine against malaria.
When I last checked the Johns Hopkins site, the total estimate of COVID-19 cases since we started keeping track have been a little less than 237 million. (Just how accurate that guess is, is another issue.)
In that time period, there have been approximately 382 million cases of malaria, a debilitating disease that cripples economies, and preferentially kills young children.
But there is good news. While there is still much room for new vaccine-development techniques to improve the situation, there is now a vaccine for malaria. It was developed by GlaxoSmithKline* and proven effective six years ago. Finally, after futher testing, has been given the green light for mass vaccinations in sub-Saharan Africa.
"Effective," in this case, is only 40%—I said there was room for improvement—and requires a series of four shots, given at five, six, seven, and 18 months of age. In a part of the world where health care is often less than stellar, I imagine this will be a challenge to implement. But malaria is a much trickier disease than, say, COVID ("comparing them is like comparing a person and a cabbage") and this is a huge milestone.
It causes all, both small and great, both rich and poor, both free and slave, to be marked on the right hand or the forehead, so that no one can buy or sell unless he has the mark. — Revelation 13:16-17
College is a time for wide-ranging, speculative discussions, and among my fellow students in the early 1970's this Bible verse was a popular topic. We were hard-pressed to imagine a world in which people would consent to having marks imposed on their bodies: tattoos were so rare that most of us had never seen one, and the now-common practice of implanting informative microchips in pets was 15 years in the future. The microchip itself had barely made any impression on our lives—my choice when doing my physics homework was between long, laborious hand calculations and a long trek through the snow to a small room where half a dozen chunky, very basic calculators had been made available to students.
Even more puzzling was how having or not having this "mark of the beast" could be the gateway to commerce. The marketplace still ran on cash and checks.
How much can change in 50 years.
Suddenly, in Canada, in Australia, in Switzerland, and in parts of the United States, the marketplace and much more are now gated by vaccination status. Society has been divided as by a sharp sword between the haves and the have-nots; the clean and the unclean; the ones who are free to travel, attend school, eat at restaurants, and even hold their jobs, and those who are not.
I am not saying that the COVID-19 vaccine is the Mark of the Beast. It seems clear that the Mark will involve some form of blasphemy and idolatrous worship, and this does not—although, frankly, the efforts to invalidate religious exemptions to vaccine mandates have me wondering a bit about that.
However, it is now crystal clear is that what seemed impossibly fanciful back in my college days is not only possible, but can sweep over even a free and democratic country with little effective opposition. Whatever that Mark may be, we have opened the door.
Our doctor's office has yet another set of forms for us to fill out, and this one just has me wanting to throw up my hands and scream, "NONE OF YOUR BUSINESS!" Plus, some of the questions make no sense, in some cases giving far more options than reasonable, and in some cases too few.
For "Ethnic Background" I am given these options:
- Ashkenazi
- No
- Other
- Unknown
I understand that there are certain diseases that are more prevalent among Ashkenazi Jews, so maybe that's an important question. But there are also diseases that are especially prevalent among other populations, e.g. the Amish, and there's no opportunity to indicate that, other than the non-informative "Other." And just who are the No people—an obscure tribe of Papua New Guinea, perhaps? And is my own diverse ancestry, which took up some dozen slots on the 2020 census form, of no medical interest at all?
One ethnicity gets its very own question:
- Hispanic or Latino/a
- Not Hispanic or Latino/a
- Unknown or Not Given
I find that a curious question for a doctor to ask. Just how many diseases divide themselves by this criterion? If my lungs are congested, how much does it matter whether my ancestors came from Spain versus France? "Not Given" is beginning to look like the best answer for most of these questions.
There's a good deal more choice when it comes to Sexual Orientation:
- Bisexual
- Choose not to disclose
- Don't know
- Lesbian or Gay
- Something else
- Straight (not lesbian or gay)
- (You can hold the CTRL key while clicking to select multiple options)
Frankly, unless I'm indicating problems of a sexual nature, I don't think even my doctor needs to know this information, though she's welcome to guess based on the fact that I'll admit to being female and having a husband. "Something else" sounds attractively bear-poking, however.
But even Sexual Orientation has nothing on Religion!
- African Methodist Episcopal
- Agnostic
- Amish
- Anglican
- Assemblies of God
- Atheist/Humanist
- Baptist
- Buddhist
- Catholic
- Christian
- Christian Scientist
- Church of Christ
- Church of Jesus Christ of Latter-day Saints
- Decline to Answer
- Disciples of Christ
- Episcopalian
- Greek Orthodox
- Haitian Vodou
- Hindu
- Indian Orthodox
- Islam
- Jain
- Jehovah's Witness
- Jewish
- Lutheran
- Mennonite
- Messianic Judiasm [that's how they spelled it]
- Methodist
- Multi-Faith
- Nazarene
- Non-Denominational
- None
- Orthodox
- Other
- Pentecostal
- Presbyterian
- Protestant
- Quaker
- Rastafarian
- Russian Orthodox
- Scientologist
- Seventh Day Adventist
- Shinto
- Sikh
- Taoist
- Unitarian Universalist
- United Church of Christ
- Unknown
- Wiccan
- Zoroastrian
There are so many things wrong with this list I won't even try to ennumerate them, other than to mention that my Seventh-Day Baptist ancestors would be feeling left out. And to note that it's just plain weird to have so many choices yet list "Islam" as one-size-fits-all. For myself, being unable to choose among Anglican, Christian, Episcopalian, Multi-Faith, Non-Denominational, Protestant, and Other—and not having the ctrl/click option for this one—I might have to go with that fascinating new religion, Decline to Answer.
But really, of what possible importance could the answer to this question be for normal medical care, other than the above-mentioned correlation between being Amish and certain diseases? Even that is an ethnic difference, not a religious one. Do Wiccans require different cancer treatments from Zoroastrians? True, Jehovah's Witnesses don't want blood transfusions, so that's important to know, but I think it would be safer and more efficient to ask that question directly, rather than make the assumption. I suspect not all JW's reject them totally, and for all I know, some other religion frowns on them as well.
Maybe these questions are required by Medicare. I have had more patience with my medical caregivers (though less with the government) ever since I learned that the very annoying questions they started asking at every visit were government-imposed: Have you fallen at all in the last year? "I have grandchildren. Falls are the natural consequence of fun." Have you been depressed during the last year? "I'm here for a physical, not a mental."
It's a good thing we like our doctors. The bureaucracy is rapidly eroding my confidence in the system.
Finally, someone—someone whose work I respect—has said what I have been saying since the beginning of the pandemic lockdowns. I'm tired of being laughed at, and much worse, when I point out that it is inconsistent to excoriate people who resist some of the anti-pandemic measures, while at the same time themselves not thinking twice about driving a car. Both are actions that can endanger others, but most of us have decided to give automobile dangers a pass. We think so little about them that we tolerate, even joke about, impaired driving, speeding, road rage, poorly-maintained cars, and driving without a license or insurance coverage. Cracking down in these areas would no doubt make a huge difference in automobile injuries and fatalities. But even then there would be dangers from weather, from carelessness, and from that wasp that flew in the window and is crawling into your ear. (The last really happened to a friend of ours, who managed to get off the road safely—I'm not sure I could have.)
You want to protect yourself and others? If you can't walk to where you are going, stay home.
But of course we don't do that. The consequences would be too great.
I want people to understand that the various measures we are taking against this pandemic also have great consequences, ones that are not as immediately obvious as ending up in a COVID hospital ward.
George Friedman says it well in his article (from which I took my own post title), COVID and Cars. Unfortunately, it is behind a pay wall, but I've extracted a few quotes.
Every year in the United States, about 40,000 people die in car accidents. Some 1.35 million die in car accidents globally. In fact, they are the eighth-largest cause of death in the world. In the United States, about 3 million people are injured in automobile-related accidents.
These numbers exist despite all the efforts made to make cars safer. The reason cars aren’t banned is because the economic and social consequences of doing so would be devastating. The supply of food and other essentials requires trucking. Maintaining friends and seeing family require cars. In the United States, our ability to use land efficiently depends on cars to sustain a dispersed population. Yet this dependency carries a risk. In the back of your mind, you are aware as the ignition is turned on that you may die. You dismiss this possibility, of course, and proceed with your life.
What has happened is that a known risk of death and injury has been measured against the necessities of life, and a calculated risk has shown that tolerating the chance of death and enjoying the benefits of the car is preferable to seeking to eliminate car deaths by eliminating the car. The principle that death must be fought by all means is not practiced in the case of car deaths because a more subtle calculation takes place.
It’s a reminder that in most actions of human life there is a possibility of death or injury, but a life without those things would be impoverished. You can live without many things for a short and predictable period. Living without them indefinitely creates pressures on individuals and society. The trade-off between death and life is the human condition.
The idea that we can go on indefinitely with each new chapter forcing us to shelter in place is a superficial view of what will happen. As with automobiles, where we risk death on every ride and where many find it, the risk of COVID-19 will be integrated into our thinking, and we will make choices.
Part 1 of the visit of our Swiss family is here, part 2 here.
At last, Christmas drew near, and we focussed our activities nearer home. Christmas Eve saw us in church, of course, with some of our guests pressed into service in our hand chime choir. Hand chimes are not nearly as beautiful as handbells, but they are what we had. We didn't even have a handbell choir until it emerged as a desperation move to give our choir a way to make music when rehearsing and singing were forbidden. In this we were oppressed, not by the state, but by our very own bishop, whose rules were far more draconian than the governments'. I had so looked forward to being able to share with our family the absolute beauty of our high church worship, especially on such a special day, but it was not allowed to be. Nonetheless, we were grateful to be permitted in-person services at all. We were there; God was there. And some of us went back later for the midnight mass.
 cropped.jpg)
.jpg)
.jpg)
Credit for the above three photos Anke Cirillo of Three Point Photography
And then it was Christmas! Happiness is a house full of family.

After Christmas we boldly got together with our long-time friend and former choir director for one of our spontaneous music-making sessions. It's impossible to describe what a glorious outpouring of joy there is in these events. I do have a few recordings I treasure, but out of respect for the true musicians who don't always appreciate having their impromptu experimentations broadcast to the world, I'll leave it to your imagination. We had singing, piano, harmonica, viola, recorder, hand chimes, and all manner of percussion. If I could do this every night I know my mental state would take a drastic turn for the better. And the interaction between me on the tambourine and our granddaughter on the maracas was pretty good physical exercise, too.
We visited several playgrounds and natural parks, including taking the Black Point Wildlife Drive on the east coast. It's a favorite of ours, and a lovely place to see birds. On this trip, however, the more exciting views were of another sort:

And what's a trip to that part of the state without a stop at the Dixie Crossroads restaurant?
We continued to enjoy our final days of this visit, trying not to think too much about the upcoming long trip to Miami and the even longer trip across the Atlantic. And the 10-day quarantine awaiting them back in Switzerland. But they survived all that without catching COVID-19, and so did we. We are so grateful to Florida for welcoming our overseas family, to Switzerland for letting them come (and return), and to all whose efforts made this visit possible. I hadn't fully realized the toll these pandemic restrictions had taken on our mental health until we were reminded of what we were missing. I believe this visit came just in time, and I'm so glad we made the joyful choice.
This December visit seems more than six months distant, given that January and February brought us vaccines and the beginning of more freedom, at least in Florida. It would be April before the Northeast opened up enough for another healing family visit ... and that's a story for another post.
Permalink | Read 4135 times | Comments (0)
Category Hurricanes and Such: [first] [previous] [next] [newest] Health: [first] [previous] [next] [newest] Politics: [first] [previous] [next] [newest] Children & Family Issues: [first] [previous] [next] [newest] Everyday Life: [first] [previous] [next] [newest]

